- Untitled.png (7.54 KiB) Viewed 3670 times
COVID-19
-
sTeamTraen
- After Pie
- Posts: 2559
- Joined: Mon Nov 11, 2019 4:24 pm
- Location: Palma de Mallorca, Spain
Re: COVID-19
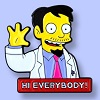
Something is going really wrong in Italy. Chart shows (X) last 30 days, (Y) Italian new cases divided by UK new cases. Much the same pattern emerges if I replace the UK figures with those from France, Germany, or the Netherlands. A month ago Italy was still being mentioned as a country that had managed to avoid getting swept up in the second wave, but now they are doing worse than many of their neighbours.
Something something hammer something something nail
-
sTeamTraen
- After Pie
- Posts: 2559
- Joined: Mon Nov 11, 2019 4:24 pm
- Location: Palma de Mallorca, Spain
Re: COVID-19
Does your dataset include the test positivity rate? My concern is that the testing system is not detecting enough cases.
Something something hammer something something nail
Re: COVID-19
From the UK gov data (link) I routinely download "PillarOneTwoTestsByPublishDate" and cross to cases by specimen date giving:sTeamTraen wrote: ↑Sun Nov 01, 2020 8:28 pmDoes your dataset include the test positivity rate? My concern is that the testing system is not detecting enough cases.
- chart (1).png (9.83 KiB) Viewed 3655 times

Re: COVID-19
No but the positivity test rate has increased:KAJ wrote: ↑Sun Nov 01, 2020 9:02 pmFrom the UK gov data (link) I routinely download "PillarOneTwoTestsByPublishDate" and cross to cases by specimen date giving:sTeamTraen wrote: ↑Sun Nov 01, 2020 8:28 pmDoes your dataset include the test positivity rate? My concern is that the testing system is not detecting enough cases.
chart (1).png
I think it's widely accepted that the testing doesn't pick up anything like all the cases, but I'm not aware of any reason to believe the proportion of detected cases has decreased.
Still the best dashboard - but *finally* HMG has something nearly as good as this part-time project by a student doing this manually.
https://www.travellingtabby.com/uk-coronavirus-tracker/
- Screenshot 2020-11-01 211612.png (63.39 KiB) Viewed 3650 times
Have you considered stupidity as an explanation
Re: COVID-19
In case you're interested, here is that chart going back to April.
- chart (3).png (9.53 KiB) Viewed 3649 times
Re: COVID-19
The number of tests hasn't increased (by much) recently...jimbob wrote: ↑Sun Nov 01, 2020 9:16 pmNo but the positivity test rate has increased:KAJ wrote: ↑Sun Nov 01, 2020 9:02 pmFrom the UK gov data (link) I routinely download "PillarOneTwoTestsByPublishDate" and cross to cases by specimen date giving:
chart (1).png
I think it's widely accepted that the testing doesn't pick up anything like all the cases, but I'm not aware of any reason to believe the proportion of detected cases has decreased.
Still the best dashboard - but *finally* HMG has something nearly as good as this part-time project by a student doing this manually.
https://www.travellingtabby.com/uk-coronavirus-tracker/
Screenshot 2020-11-01 211612.png
- chart (4).png (8.09 KiB) Viewed 3646 times
WRT data summary/analysis, I've no decent software since retirement so I'm using Google Sheets, but I have ImportData() links to the HMG data which automagically import the latest data and update charts etc.
-
Bird on a Fire

- Princess POW
- Posts: 10142
- Joined: Fri Oct 11, 2019 5:05 pm
- Location: Portugal
Re: COVID-19
Woah, that's a huge increase in the positivity rate - is that both pillars?jimbob wrote: ↑Sun Nov 01, 2020 9:16 pmNo but the positivity test rate has increased:KAJ wrote: ↑Sun Nov 01, 2020 9:02 pmFrom the UK gov data (link) I routinely download "PillarOneTwoTestsByPublishDate" and cross to cases by specimen date giving:sTeamTraen wrote: ↑Sun Nov 01, 2020 8:28 pmDoes your dataset include the test positivity rate? My concern is that the testing system is not detecting enough cases.
chart (1).png
I think it's widely accepted that the testing doesn't pick up anything like all the cases, but I'm not aware of any reason to believe the proportion of detected cases has decreased.
Still the best dashboard - but *finally* HMG has something nearly as good as this part-time project by a student doing this manually.
https://www.travellingtabby.com/uk-coronavirus-tracker/
I can see why the % positive would increase in Pillar 1 if more NHS workers are getting infected (though hopefully not), but not Pillar 2. The number of negative Pillar 2 tests (people with covid symptoms but who test negative) should be roughly stable or even increasing (more winter colds etc), with the increase in covid cases coming on top of that.
Either they've suddenly found a more accurate way to screen people before administering a test, or the testing is getting overwhelmed again.
We have the right to a clean, healthy, sustainable environment.
-
Bird on a Fire
- Princess POW
- Posts: 10142
- Joined: Fri Oct 11, 2019 5:05 pm
- Location: Portugal
Re: COVID-19
Well as noted above, it happened during the first wave https://www.medrxiv.org/content/10.1101 ... 20128777v1 I'm not quite sure why you'd expect it to be different this time around.KAJ wrote: ↑Sun Nov 01, 2020 9:02 pmFrom the UK gov data (link) I routinely download "PillarOneTwoTestsByPublishDate" and cross to cases by specimen date giving:sTeamTraen wrote: ↑Sun Nov 01, 2020 8:28 pmDoes your dataset include the test positivity rate? My concern is that the testing system is not detecting enough cases.
chart (1).png
I think it's widely accepted that the testing doesn't pick up anything like all the cases, but I'm not aware of any reason to believe the proportion of detected cases has decreased.
We have the right to a clean, healthy, sustainable environment.
-
sTeamTraen
- After Pie
- Posts: 2559
- Joined: Mon Nov 11, 2019 4:24 pm
- Location: Palma de Mallorca, Spain
Re: COVID-19
Have you considered learning R? It's free, and very powerful.
Something something hammer something something nail
Re: COVID-19
At first glance Screenshot 2020-11-01 211612.png looks like the HMG data from whichBird on a Fire wrote: ↑Sun Nov 01, 2020 9:40 pmWoah, that's a huge increase in the positivity rate - is that both pillars?jimbob wrote: ↑Sun Nov 01, 2020 9:16 pmNo but the positivity test rate has increased:
Still the best dashboard - but *finally* HMG has something nearly as good as this part-time project by a student doing this manually.
https://www.travellingtabby.com/uk-coronavirus-tracker/
Screenshot 2020-11-01 211612.png
I can see why the % positive would increase in Pillar 1 if more NHS workers are getting infected (though hopefully not), but not Pillar 2. The number of negative Pillar 2 tests (people with covid symptoms but who test negative) should be roughly stable or even increasing (more winter colds etc), with the increase in covid cases coming on top of that.
Either they've suddenly found a more accurate way to screen people before administering a test, or the testing is getting overwhelmed again.
1 August
newPillarOneTwoTestsByPublishDate 130,999
newCasesBySpecimenDate 542
positivity rate = 542/130999 = 0.41%
29 October
newPillarOneTwoTestsByPublishDate 317,247
newCasesBySpecimenDate 19,525
positivity rate =19,525/317,247 = 6.15%
It's widely accepted that the real number of cases has increased a lot in the last few months, now reflected in hospitalisations, ventilator beds, and deaths. I don't see why the increased positivity rate cannot be explained by an increase in the real number of cases. I don't see any reason to invoke a change in the proportion of real cases which are detected. Can you point me to a reason?
I haven't read all the posts in this thread and can't remember all those I've read (I'm getting old!). If "as noted above" means an earlier post, can you point me to it?Bird on a Fire wrote: ↑Sun Nov 01, 2020 9:45 pmWell as noted above, it happened during the first wave https://www.medrxiv.org/content/10.1101 ... 20128777v1 I'm not quite sure why you'd expect it to be different this time around.
That link is to a 45 page preprint. The abstract doesn't mention that the proportion of the real number of cases which was detected decreased and it'll be some time before I have time to read the whole paper. Can you point me to the relevant section, or even summarise the argument?
I'm very ready to believe I've missed something, it happens often
Re: COVID-19
Thanks, and yes, I used R extensively before retirement (even had one fix accepted by R-core, immortalitysTeamTraen wrote: ↑Sun Nov 01, 2020 10:15 pmHave you considered learning R? It's free, and very powerful.
-
Bird on a Fire
- Princess POW
- Posts: 10142
- Joined: Fri Oct 11, 2019 5:05 pm
- Location: Portugal
Re: COVID-19
Ah sorry, it wasn't above but the previous pageKAJ wrote: ↑Sun Nov 01, 2020 10:37 pmI haven't read all the posts in this thread and can't remember all those I've read (I'm getting old!). If "as noted above" means an earlier post, can you point me to it?Bird on a Fire wrote: ↑Sun Nov 01, 2020 9:45 pmWell as noted above, it happened during the first wave https://www.medrxiv.org/content/10.1101 ... 20128777v1 I'm not quite sure why you'd expect it to be different this time around.
That link is to a 45 page preprint. The abstract doesn't mention that the proportion of the real number of cases which was detected decreased and it'll be some time before I have time to read the whole paper. Can you point me to the relevant section, or even summarise the argument?
I'm very ready to believe I've missed something, it happens often
Note that this paper is a few months old now. I don't know if anybody is regularly assimilating the different data sources every week or so, but it would be useful to confirm what's going on with the numbers everybody is relying on to make decisions.Bird on a Fire wrote: ↑Sat Oct 31, 2020 2:56 pmThere's between a third and a half as many Pillar 1 (NHS/PHE) tests as Pillar 2 (partner labs), depending on the week, and the latter are only given to people already showing symptoms.
This is a known issue in the data, btw, or at least people who've actually run the numbers have identified it too.
For example, one of PeteB's links a few pages back linked to this preprint https://www.medrxiv.org/content/10.1101 ... 20128777v1 comparing different data sources during the first wave via a data assimilation technique borrowed from geosciences. What they call 'experiment DH' was a model using deaths and hospitalisation data only to model the progress of the epidemic in England.
I know there's more tests available now, but still not enough, so it seems reasonable to assume that the proportion of cases identified varies as a function of the number of cases in a way that systematically underestimates case number.As discussed in Section 5.1, the reported number of cases testing positive for SARS-Cov-2
underestimates significantly the actual number of people infected by the virus. We can assess the
magnitude of this underestimation by comparing the number of cases predicted by experiment DH
to the reported number of cases. We find that as the number of people infected grew exponentially
before the lockdown started and the reproduction number declined to below 1.0, the percentage
of positive cases not being reported increased due to a severe lack of testing kits. On March
25th, this number peaked, with reporting of only 1% of cases. As more tests became available,
and simultaneously the rate of infection reduced, the percentage of unreported cases decreased.
From the beginning of May, about 2% of the accumulated cases are reported. The UK government
achieved its self-imposed target of 100,000 tests per day for the first time on May 1st. The estimated
percentage of reported cases can be compared to the percentage of asymptomatic cases. Estimates
of the proportion of asymptomatic cases vary widely between studies. However, WHO suggests
that 80% of infections are mild or asymptomatic [61], supported by [34]. Therefore, due to the
testing strategy in the UK (only testing people displaying symptoms), we could conclude that
approximately 10% of the accumulated symptomatic cases are being reported from the beginning
of May.
We have the right to a clean, healthy, sustainable environment.
-
sTeamTraen
- After Pie
- Posts: 2559
- Joined: Mon Nov 11, 2019 4:24 pm
- Location: Palma de Mallorca, Spain
Re: COVID-19
https://blog.sellorm.com/2018/12/20/ins ... hromebook/KAJ wrote: ↑Sun Nov 01, 2020 10:42 pmThanks, and yes, I used R extensively before retirement (even had one fix accepted by R-core, immortality). Not only have I no decent software, I have no decent hardware - I'm using a Chromebook. I'm aware of rdrr.io/snippets/ but that isn't really suitable for this kind of thing.
Something something hammer something something nail
Re: COVID-19
I seem to be the resident doom monger in our dance scene - I'm still going to rehearsals for the (small) performance troupe but I've avoided teaching group classes or going to social dance events, even though there is currently no covid in the state because I can't think of an activity better suited to spreading a respiratory disease. Right now, dancing in Tasmania strikes me as an activity that's really safe right up to the moment that it's not. Our quarantine system has been working amazingly but "essential workers" are exempt from it, so we can't expect it to be perfect.headshot wrote: ↑Thu Oct 29, 2020 11:34 amCrazy isn't it?shpalman wrote: ↑Thu Oct 29, 2020 11:10 amThat's the one which said "Tourism is the life blood, so I'm not surprised the SC & Doc issued the exemption for more than 1500 dancers" and "It’s hard to believe that so many Dancers have Covid-19 after going to a Dance Event"?
Who would have guessed that lots of people would catch a aerosol- and contact-contagious disease from each other in an event characterized by physical exertion and close contact! Even after they had been given an exemption!
And so, even in our (presumably) covid-free environment, not dancing feels like the smallest of sacrifices I could make towards avoiding super-spreader events. I don't feel quite strongly enough to argue to publicly about it, I'm just choosing not to participate. If I were in Europe or the US, I would find it very hard not to shout at people for being dangerous idiots.
-
Woodchopper

- Princess POW
- Posts: 7163
- Joined: Sat Oct 12, 2019 9:05 am
Re: COVID-19
South Korea has one of the best records in dealing with the pandemic. Despite being one of the first countries affected after China, it has experienced less than 300 deaths in total.
This has been achieved through:
The rest of the article is open access and interesting.
This has been achieved through:
https://bmcmedicine.biomedcentral.com/a ... 20-01791-8This analysis of South Korea’s response to COVID-19 highlights how, despite a sharp growth in cases early in the pandemic, transmission was rapidly controlled, resulting in a relatively small epidemic made up of large linked clusters. The Shincheonji religious group cluster accounted for 39% of all cases. We estimate Rt to have been brought below one in April, and although estimates rose above one during May and early June, this reflected transmissibility within highly localised clusters rather than widespread national transmission. As of July 13th, 13,479 cases and 289 deaths have been reported since the first case on January 20th [2]. The rapid expansion of test capacity, early localised strengthening of social distancing measures in Daegu, voluntary reduction in movement prior to the mandated enhanced national social distancing campaign, and continued case-based contact tracing across the large clusters in Seoul Metropolitan Region have all likely contributed to help contain South Korea’s epidemic.
South Korea has not implemented a national lockdown. Instead, the comprehensive approach ranges from case-based testing and isolation, investigation of large clusters of confirmed cases, and short, targeted strong social distancing measures in the most heavily affected regions. Early identification and management of cases, clusters, and contacts have been a key strategy of the South Korea response. Combined with the expanded testing capacity, the use of mass testing in high-risk facilities and clusters has allowed the majority of new cases to be traced back to existing clusters (Fig. 5), such as the Shincheonji religious group, a call centre in Seoul, healthcare institutions in Daegu, and the Itaewon nightclubs.
[...]
Like other countries looking at exiting their lockdowns, the long-term strategy in South Korea involves a mix of social distancing policies, behavioural interventions, and testing. South Korea moved to a phase of partially relaxed social distancing on May 6th [34]. This included allowing activities in low-risk venues (e.g. recreation parks, forests, closed-door sporting events) while maintaining partial restrictions on the use of high-risk facilities (e.g. religious facilities, fitness venues) and non-essential public gatherings which are all subject to strict infection prevention and control guidelines [33]. Additionally, schools reopened in late May and a growing number of companies have eased their “smart-working” policies [12, 14, 48]. Consultations between government, industry, and community-based bodies have been conducted to increase preparedness, reduce conflicts, and maximise uptake of long-term “every day” social distancing [78].
It is important to emphasise some key aspects particular to the outbreak in South Korea, which are relevant when attempting to apply lessons to other settings. The number of SARS-CoV-2 infections in South Korea has been far smaller than the USA or most European countries. Over two thirds of cases were linked to a few major clusters, which were promptly identified and tested en masse. South Korea has implemented effective strategies for detecting and quarantining imported cases, reducing the risk of secondary transmission. All these measures have contributed to the outbreak remaining geographically localised. However, cluster-based management will be more difficult in settings with much more widespread transmission. Finally, the South Korean response was facilitated by structures and processes such as additional legal powers for quarantine, surveillance systems, and digital technologies introduced after the 2015 Middle East respiratory syndrome (MERS) outbreak [79] which may be lacking in other countries. These key aspects may limit the extent to which the testing and contact tracing strategies adopted by South Korea can be translated to other settings.
The rest of the article is open access and interesting.
-
FlammableFlower
- Dorkwood
- Posts: 1520
- Joined: Mon Nov 11, 2019 1:22 pm
Re: COVID-19
Not sure where to put this... but here's Farage adding to the stupidity...:
f.ckwitNigel Farage was equally critical of the new restrictions announced by Prime Minister Boris Johnson over the weekend. In an opinion piece published Sunday in the Telegraph, he said that he planned to relaunch his party as an anti-lockdown group called Reform UK that will back a controversial strategy to pursue “herd immunity” by protecting only the most vulnerable.
-
El Pollo Diablo

- Stummy Beige
- Posts: 3355
- Joined: Wed Sep 25, 2019 4:41 pm
- Location: FBPE
Re: COVID-19
Blair was on R4 this morning. His points about Covid were:
- Optimism about being able to deal with the virus by Spring, but worry is between now and then
- Use November to do four things:
1. Look at accelerating deployment of vaccines, because trials are showing the AstraZeneca vaccine is safe, the question that remains is around effectiveness - if they're over 40-50% effective they should be deployed regardless of the exact effectiveness number.
2. For therapeutics, new monoclodal antibody therapeutic drugs - provided they're safe, look at how to accelerate the deployment of those so they're available before Christmas. Extend the Recovery trial, to get more people the opportunity to get lifesaving drugs, particularly in the early stages of treatment.
3. Testing - appoint a minister and team whose sole job is to do nothing other than ensure every university tests every student before they return for the winter holidays, and do the same with schools.
4. Data - get the best data system from around the world, and put it in place.
November should be the month for organisation and preparation, which might allow opening up in December.
The presenter pushed back on the trial suggestions, saying that if they're widened we might not know what happens. Blair said that if there's a question of safety then that's a red line, but holding back treatments from people where you think there's a chance of helping is a problem.
Full interview from 2:49:10 here. Any thoughts?
- Optimism about being able to deal with the virus by Spring, but worry is between now and then
- Use November to do four things:
1. Look at accelerating deployment of vaccines, because trials are showing the AstraZeneca vaccine is safe, the question that remains is around effectiveness - if they're over 40-50% effective they should be deployed regardless of the exact effectiveness number.
2. For therapeutics, new monoclodal antibody therapeutic drugs - provided they're safe, look at how to accelerate the deployment of those so they're available before Christmas. Extend the Recovery trial, to get more people the opportunity to get lifesaving drugs, particularly in the early stages of treatment.
3. Testing - appoint a minister and team whose sole job is to do nothing other than ensure every university tests every student before they return for the winter holidays, and do the same with schools.
4. Data - get the best data system from around the world, and put it in place.
November should be the month for organisation and preparation, which might allow opening up in December.
The presenter pushed back on the trial suggestions, saying that if they're widened we might not know what happens. Blair said that if there's a question of safety then that's a red line, but holding back treatments from people where you think there's a chance of helping is a problem.
Full interview from 2:49:10 here. Any thoughts?
If truth is many-sided, mendacity is many-tongued

Re: COVID-19
I thought that racist actor had already launched a new party called Reform or Relate or Retain or something? Not sure that Putin wants to fund every new party these con artists set up.FlammableFlower wrote: ↑Mon Nov 02, 2020 10:40 amNot sure where to put this... but here's Farage adding to the stupidity...:f.ckwitNigel Farage was equally critical of the new restrictions announced by Prime Minister Boris Johnson over the weekend. In an opinion piece published Sunday in the Telegraph, he said that he planned to relaunch his party as an anti-lockdown group called Reform UK that will back a controversial strategy to pursue “herd immunity” by protecting only the most vulnerable.
 Awarded gold star 4 November 2021
Awarded gold star 4 November 2021-
Little waster

- After Pie
- Posts: 2385
- Joined: Tue Nov 12, 2019 12:35 am
- Location: About 1 inch behind my eyes
Re: COVID-19
FlammableFlower wrote: ↑Mon Nov 02, 2020 10:40 amNot sure where to put this... but here's Farage adding to the stupidity...:f.ckwitNigel Farage was equally critical of the new restrictions announced by Prime Minister Boris Johnson over the weekend. In an opinion piece published Sunday in the Telegraph, he said that he planned to relaunch his party as an anti-lockdown group called Reform UK that will back a controversial strategy to pursue “herd immunity” by protecting only the most vulnerable.
That would be the "herd immunity" we are now pretty certain COVID infections don't meaningfully provide.
I for one am shocked to find Farage pushing his lunatic far-right beliefs regardless of trivial things like observable reality or any scientific understanding, I imagine this approach is completely uncharacteristic for him and totally without precedent.
This place is not a place of honor, no highly esteemed deed is commemorated here, nothing valued is here.
What is here was dangerous and repulsive to us.
This place is best shunned and left uninhabited.
What is here was dangerous and repulsive to us.
This place is best shunned and left uninhabited.
-
discovolante

- Stummy Beige
- Posts: 4117
- Joined: Fri Oct 11, 2019 5:10 pm
Re: COVID-19
Well it does sorta make me wish Tony Blair was still PM.El Pollo Diablo wrote: ↑Mon Nov 02, 2020 10:57 amBlair was on R4 this morning. His points about Covid were:
- Optimism about being able to deal with the virus by Spring, but worry is between now and then
- Use November to do four things:
1. Look at accelerating deployment of vaccines, because trials are showing the AstraZeneca vaccine is safe, the question that remains is around effectiveness - if they're over 40-50% effective they should be deployed regardless of the exact effectiveness number.
2. For therapeutics, new monoclodal antibody therapeutic drugs - provided they're safe, look at how to accelerate the deployment of those so they're available before Christmas. Extend the Recovery trial, to get more people the opportunity to get lifesaving drugs, particularly in the early stages of treatment.
3. Testing - appoint a minister and team whose sole job is to do nothing other than ensure every university tests every student before they return for the winter holidays, and do the same with schools.
4. Data - get the best data system from around the world, and put it in place.
November should be the month for organisation and preparation, which might allow opening up in December.
The presenter pushed back on the trial suggestions, saying that if they're widened we might not know what happens. Blair said that if there's a question of safety then that's a red line, but holding back treatments from people where you think there's a chance of helping is a problem.
Full interview from 2:49:10 here. Any thoughts?
To defy the laws of tradition is a crusade only of the brave.
Re: COVID-19
Oooh! Thanks for thatsTeamTraen wrote: ↑Sun Nov 01, 2020 11:05 pmhttps://blog.sellorm.com/2018/12/20/ins ... hromebook/KAJ wrote: ↑Sun Nov 01, 2020 10:42 pmThanks, and yes, I used R extensively before retirement (even had one fix accepted by R-core, immortality
-
shpalman

- Princess POW
- Posts: 8341
- Joined: Mon Nov 11, 2019 12:53 pm
- Location: One step beyond
- Contact:
Re: COVID-19
Don't know, it looks fine if I plot Italian new cases divided by Italian new cases.sTeamTraen wrote: ↑Sun Nov 01, 2020 8:26 pmSomething is going really wrong in Italy. Chart shows (X) last 30 days, (Y) Italian new cases divided by UK new cases. Much the same pattern emerges if I replace the UK figures with those from France, Germany, or the Netherlands. A month ago Italy was still being mentioned as a country that had managed to avoid getting swept up in the second wave, but now they are doing worse than many of their neighbours.
Untitled.png
It only looks bad if I just plot the number of Italian new cases.
having that swing is a necessary but not sufficient condition for it meaning a thing
@shpalman@mastodon.me.uk
@shpalman@mastodon.me.uk
Re: COVID-19
Thanks for that. I'll follow it up when I have time - it looks interesting.Bird on a Fire wrote: ↑Sun Nov 01, 2020 10:50 pmAh sorry, it wasn't above but the previous pageKAJ wrote: ↑Sun Nov 01, 2020 10:37 pmI haven't read all the posts in this thread and can't remember all those I've read (I'm getting old!). If "as noted above" means an earlier post, can you point me to it?Bird on a Fire wrote: ↑Sun Nov 01, 2020 9:45 pm
Well as noted above, it happened during the first wave https://www.medrxiv.org/content/10.1101 ... 20128777v1 I'm not quite sure why you'd expect it to be different this time around.
That link is to a 45 page preprint. The abstract doesn't mention that the proportion of the real number of cases which was detected decreased and it'll be some time before I have time to read the whole paper. Can you point me to the relevant section, or even summarise the argument?
I'm very ready to believe I've missed something, it happens often
Note that this paper is a few months old now. I don't know if anybody is regularly assimilating the different data sources every week or so, but it would be useful to confirm what's going on with the numbers everybody is relying on to make decisions.Bird on a Fire wrote: ↑Sat Oct 31, 2020 2:56 pmThere's between a third and a half as many Pillar 1 (NHS/PHE) tests as Pillar 2 (partner labs), depending on the week, and the latter are only given to people already showing symptoms.
This is a known issue in the data, btw, or at least people who've actually run the numbers have identified it too.
For example, one of PeteB's links a few pages back linked to this preprint https://www.medrxiv.org/content/10.1101 ... 20128777v1 comparing different data sources during the first wave via a data assimilation technique borrowed from geosciences. What they call 'experiment DH' was a model using deaths and hospitalisation data only to model the progress of the epidemic in England.
I know there's more tests available now, but still not enough, so it seems reasonable to assume that the proportion of cases identified varies as a function of the number of cases in a way that systematically underestimates case number.quote snipped
I suppose the pillar 1/2 test subjects are not representative of the UK population, so that data positivity rate isn't a good estimate of the population positivity rate, that isn't its purpose. I guess the pillar 1/2 tests are biased towards likely cases so that data positivity rate is likely an overestimate of that in the population. But we don't have to guess; the ONS (link) do weekly random surveys intended to estimate population positivity rates. When/if I get time I'll try comparing the pillar 1/2 data with the ONS data.
-
shpalman
- Princess POW
- Posts: 8341
- Joined: Mon Nov 11, 2019 12:53 pm
- Location: One step beyond
- Contact:
Re: COVID-19
It shocks me that we were allowed to do it at all in September and October at all. It's clear that as soon as one infectious person shows up in the group, that's going to be it for the whole group.Squeak wrote: ↑Mon Nov 02, 2020 4:46 amI seem to be the resident doom monger in our dance scene - I'm still going to rehearsals for the (small) performance troupe but I've avoided teaching group classes or going to social dance events, even though there is currently no covid in the state because I can't think of an activity better suited to spreading a respiratory disease. Right now, dancing in Tasmania strikes me as an activity that's really safe right up to the moment that it's not. Our quarantine system has been working amazingly but "essential workers" are exempt from it, so we can't expect it to be perfect.headshot wrote: ↑Thu Oct 29, 2020 11:34 amCrazy isn't it?shpalman wrote: ↑Thu Oct 29, 2020 11:10 amThat's the one which said "Tourism is the life blood, so I'm not surprised the SC & Doc issued the exemption for more than 1500 dancers" and "It’s hard to believe that so many Dancers have Covid-19 after going to a Dance Event"?
Who would have guessed that lots of people would catch a aerosol- and contact-contagious disease from each other in an event characterized by physical exertion and close contact! Even after they had been given an exemption!
And so, even in our (presumably) covid-free environment, not dancing feels like the smallest of sacrifices I could make towards avoiding super-spreader events. I don't feel quite strongly enough to argue to publicly about it, I'm just choosing not to participate. If I were in Europe or the US, I would find it very hard not to shout at people for being dangerous idiots.
At the weekend there was a demonstration in Milan from (the people who run / are involved with) dance schools, gyms, and swimming pools, complaining about being shut down.
Yes you can complain about the lack of support, that's legitimate, although if your entire livelihood is based on an associazione sportiva dilettantistica you're kind of stretching the definition of dilettantistica. What you can't do is complain about being closed.
Someone from one of the dance schools was complaining that they shouldn't be subjected to the same rules as gyms and swimming pools... and the voice-over only slightly awkwardly pointed out that also people running gyms and swimming pools were also there. "Yeah but we're not like the others we deserve special treatment" says everybody. Contact sports definitely aren't safe - one of the local basketball teams (one of the best in Italy) has eight covids and is struggling to get together enough non-covid players to form a team.
I've got no patience either for the restaurant owners who are protesting about not being able to stay open, as if being open when everyone is either dead or in quarantine will see them earning enough to keep going.
"There was only was case associated with going to the theatre between mid-June and mid-October" - but there wasn't really any covid around in that period either; towards the end of October there was an outbreak in the choir of La Scala.
It seems anyone who isn't allowed to work is protesting, but then anyone who is obliged to go to work is also protesting. And the stupid breaky-stuff kids get involved and start trashing shops in the name of protecting businesses. Meanwhile fake news circulates that the hospitals are actually completely empty.
having that swing is a necessary but not sufficient condition for it meaning a thing
@shpalman@mastodon.me.uk
@shpalman@mastodon.me.uk
-
Bird on a Fire
- Princess POW
- Posts: 10142
- Joined: Fri Oct 11, 2019 5:05 pm
- Location: Portugal
Re: COVID-19
Yes, I don't think the positivity rate on its own tells us much, without also considering the number of tests conducted. In this case, the number of tests has been pretty much constant over the last month, while the % positive has ~tripled.KAJ wrote: ↑Mon Nov 02, 2020 2:31 pmI suppose the pillar 1/2 test subjects are not representative of the UK population, so that data positivity rate isn't a good estimate of the population positivity rate, that isn't its purpose. I guess the pillar 1/2 tests are biased towards likely cases so that data positivity rate is likely an overestimate of that in the population. But we don't have to guess; the ONS (link) do weekly random surveys intended to estimate population positivity rates. When/if I get time I'll try comparing the pillar 1/2 data with the ONS data.
7 day averages (from Travelling Tabby dashboard. I just chose the most recent month of data)
2nd Oct: 6273 new cases/ 232195 tests = 0.027% positive
2nd Nov: 22739 new cases / 271031 tests = 0.084% positive
The ONS data shows a similar increase in positives in the community, from 0.3% on 25 Sept to 1.1% on 23 Oct, i.e. in both cases roughly tripling.
The tested population is "people with covid symptoms", most of whom are experiencing those symptoms for some other reason. My intuition is that the number of people with symptoms who test negative should be stable, or possibly increasing with the onset of winter colds etc.
That does seem to be consistent with the data as it stands, as the increase in the number of tests is bigger than the number of cases. That said, it's not helpful having all the different pillars mixed in together as they change at different rates and measure different things. Ideally we'd be able to get data just for Pillar 2 and hard numbers for positive, negative and void - I couldn't find that info on the ONS site, is it available anywhere?
We have the right to a clean, healthy, sustainable environment.