Re: COVID-19
Posted: Tue Mar 23, 2021 4:37 pm
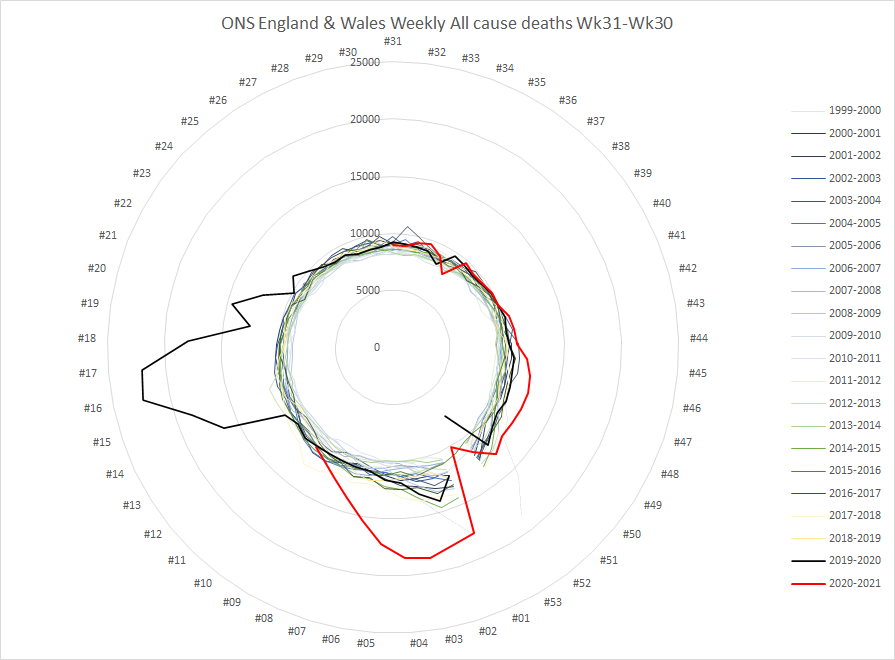
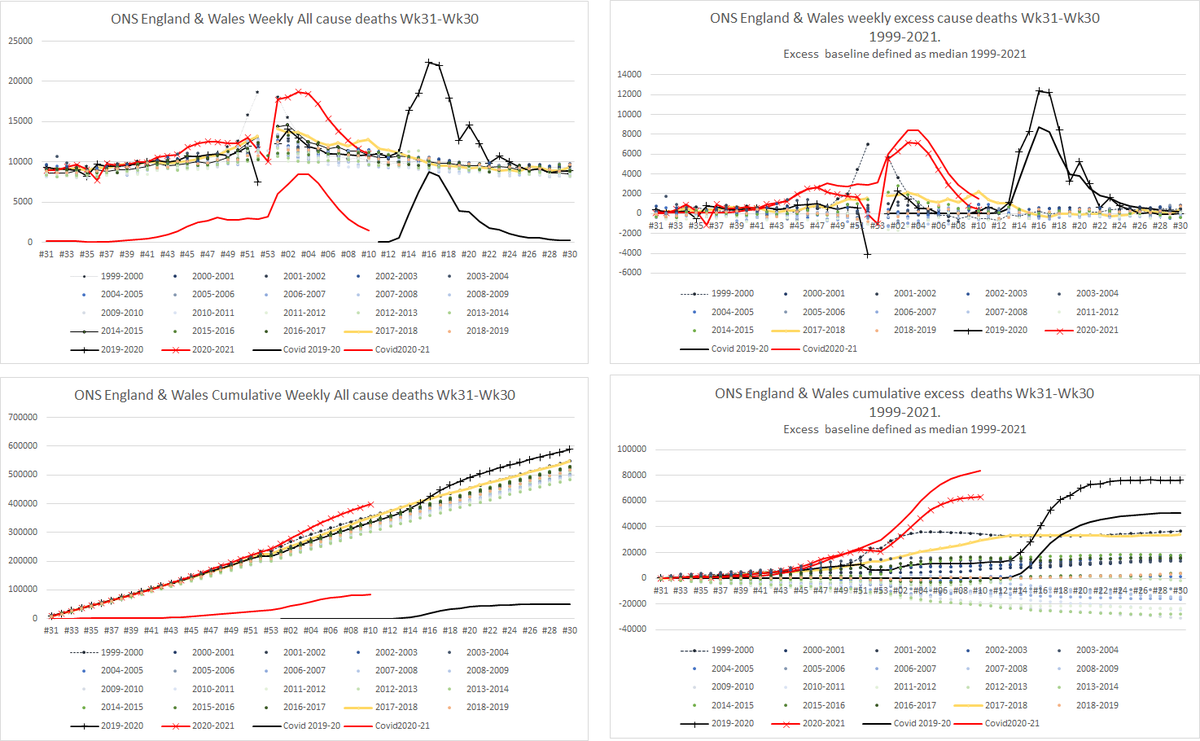
Because the 1999-201x data is from the ONS excess winter mortality report (2015-16 for example) and that all cause death data (fig 4 which you can download but will need to rename to open in excel due to filename length limits) starts in wk31, 1999.
Yup - the whole "we're 4-weeks behind Italy" which was obviously wrong at the time. If your model says that, but the deaths data (which is inherently more robust than testing data, which relies on sampling bias) shows us tracking Italy 11 days behind, it's not reality that's wrong.badger wrote: ↑Wed Mar 24, 2021 7:14 amIn among all the understandable and deserved ire directed yesterday at Boris and his cronies commemorating a disaster partly of their own making, James Annan was also getting annoyed at the subtle but telling rewriting of history with respect to Sage and I think it's worth reading in full, because it does remind us it's not all Boris's fault (first lockdown).
http://julesandjames.blogspot.com/2021/ ... aking.html
When the enquiry does finally come it won't be pretty.
I certainly remember the bafflement on here and everywhere else about the delay in locking down, and I wonder if we'll ever get to the bottom of it, or find a way of minimizing those kind of errors in the brains trust advising the country (where they are apparently so out of step with reality).
It means I can plot the data like this. Top are weekly numbers. Bottom are cumulative numbers. Left are raw numbers. Right are excess (from baseline of median 1999-2021 for that week number)
Well Switzerland or Czechia would be the poster children for this. Switzerland with the opening of ski resorts last autumn.badger wrote: ↑Mon Mar 22, 2021 2:21 pmIn the article he gives specific reasons for not using Den/Nor and non-Euro as comparators (mainly because of amount of international travel and/or climate), and am happy to go with that for the sake of argument and see what turns up...jimbob wrote: ↑Mon Mar 22, 2021 12:09 pmSweden, Denmark, Norway say that's bollocks.badger wrote: ↑Mon Mar 22, 2021 11:37 amApparently earlier does not necessarily mean better, when it comes to UK lockdown (because earlier first spring lockdown equals bigger second waves around winter, which, erm, could be prevented by, erm, earlier lockdowns?) Odd piece, seems to be no paper behind it:
Argues Cambridge Epidemiologist
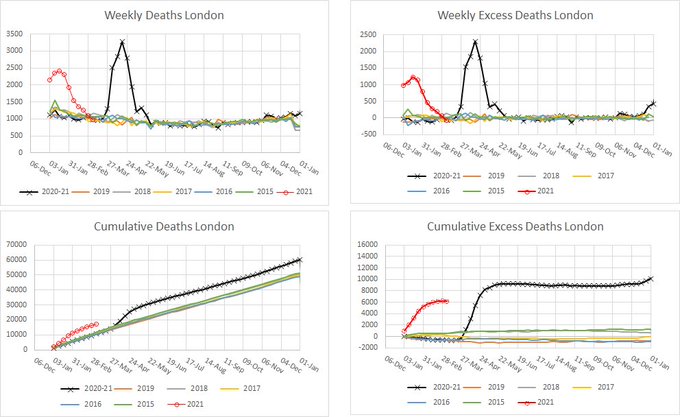
And look at London in the first and second waves too
London - yep, that seems to run counter to his argument. Sweden, am not so sure - as I see it they had a slightly higher peak of excess death in second wave, so to me that also undoes his position, but he's really talking about countries which did well first, then didn't.
Yes, but they started rising before schools went back - when mass testing of pupils started in fact.
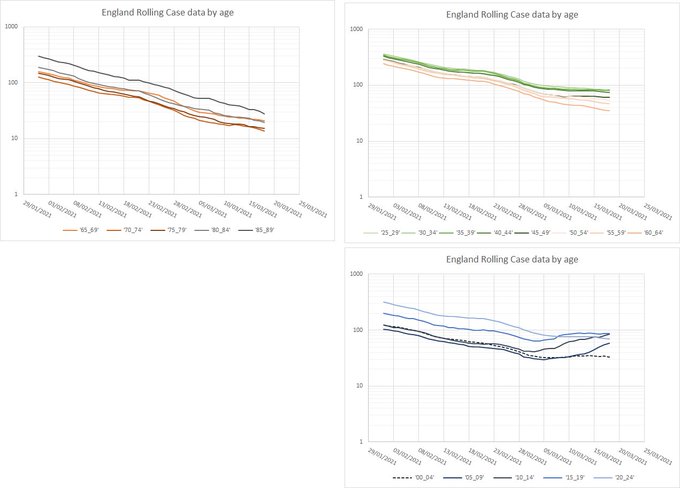
Hospital admissions are still declining in an almost pure exponential (with a small day-of-week effect) - my earlier suspicion of a flattening wasn't supported by subsequent data.Grumble wrote: ↑Wed Mar 24, 2021 7:11 pmYes, but they started rising before schools went back - when mass testing of pupils started in fact.jimbob wrote: ↑Wed Mar 24, 2021 5:56 pmMy plot of February and March cases in England according to demographics, from the government's dashboard
<snip plot>
Grouped by "mostly retired" "mostly working age" "mostly children and university age"
Cases are rising in school children - especially secondary schools
Code: Select all
At 20/03 fit = 346.4 with halving time = 17.4 days. That time doubling in 701.7 days
Analysis of Variance Table
Response: log(Admits)
Df Sum Sq Mean Sq F value Pr(>F)
poly(date, 2) 2 10.4723 5.2361 1705.7153 < 2.2e-16 ***
day 6 0.0832 0.0139 4.5146 0.001918 **
Residuals 33 0.1013 0.0031
---
Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1
Coefficients:
Estimate Std. Error t value Pr(>|t|)
(Intercept) 6.69408 0.02272 294.594 < 2e-16 ***
poly(date, 2)1 -3.22071 0.05618 -57.333 < 2e-16 ***
poly(date, 2)2 0.02417 0.05542 0.436 0.66563
dayMon 0.08806 0.03200 2.752 0.00955 **
dayTue 0.09462 0.03202 2.955 0.00574 **
dayWed 0.07673 0.03207 2.393 0.02257 *
dayThu 0.09033 0.03212 2.812 0.00822 **
dayFri 0.01038 0.03219 0.322 0.74918
daySat -0.01370 0.03227 -0.424 0.67401
---
Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1
Residual standard error: 0.05541 on 33 degrees of freedom
Multiple R-squared: 0.9905Most epidemics disappear once populations achieve herd immunity and the pathogen has too few vulnerable bodies available as hosts for its self-propagation. This herd protection comes about through the combination of natural immunity in people who’ve recovered from infection and vaccination of the remaining population.
In the case of SARS-CoV-2, however, recent developments suggest that we may never achieve herd immunity. Even the U.S., which leads most other countries in vaccinations and already had large outbreaks, won’t get there. That’s the upshot of an analysis by Christopher Murray at the University of Washington and Peter Piot at the London School of Hygiene and Tropical Medicine.
Get used to masks and physical distancing and rotating lockdowns, closed borders, fewer pubs and restos, an absence of social events. The future is now.If this is the evolutionary trajectory of SARS-CoV-2, we’re in for seemingly endless cycles of outbreaks and remissions, social restrictions and relaxations, lockdowns and reopenings. At least in rich countries, we will probably get vaccinated a couple of times a year, against the latest variant in circulation, but never fast or comprehensively enough to achieve herd immunity.
https://twitter.com/dgurdasani1/status/ ... 46724?s=19
She undoes a lot of good work there by being wrong about primary kids.shpalman wrote: ↑Thu Mar 25, 2021 7:08 amhttps://twitter.com/dgurdasani1/status/ ... 46724?s=19
A couple of things that explanation misses...
It's not too easy to see as they generally lump both into pillar 2 as far as I can tell, except for the first bit of data
I don't know if anyone in authority is planing it this way, but it seems to me what will happen is that reopening schools and relaxing lockdown will allow the disease to spread rapidly in the unvaccinated younger people in the population, presumably giving them immunity. Combined with immunity in older people from the vaccine, it's quite possible we will achieve herd immunity. Of course this depends on people spreading the disease quickly enough so that it doesn't die out leaving large pockets of people who have neither caught it nor been vaccinated. Hopefully such people would eventually be vaccinated, though it would be morally dubious to use vaccines on them which could be sent to parts of the world where lots of people are still dying of the disease.
I am not at all convinced this or will be the case. Most of the variants of concern arose prior to the vaccines being rolled. In almost all countries, there is still, insufficient people vaccination to put significant selection pressure on the virus.Herainestold wrote: ↑Thu Mar 25, 2021 12:45 amThe rapid rise of variants and rising infections in the face of vaccine rollout might mean we are now in a permanent pandemic where things will never go back to normal.
Most epidemics disappear once populations achieve herd immunity and the pathogen has too few vulnerable bodies available as hosts for its self-propagation. This herd protection comes about through the combination of natural immunity in people who’ve recovered from infection and vaccination of the remaining population.
In the case of SARS-CoV-2, however, recent developments suggest that we may never achieve herd immunity. Even the U.S., which leads most other countries in vaccinations and already had large outbreaks, won’t get there. That’s the upshot of an analysis by Christopher Murray at the University of Washington and Peter Piot at the London School of Hygiene and Tropical Medicine.Get used to masks and physical distancing and rotating lockdowns, closed borders, fewer pubs and restos, an absence of social events. The future is now.If this is the evolutionary trajectory of SARS-CoV-2, we’re in for seemingly endless cycles of outbreaks and remissions, social restrictions and relaxations, lockdowns and reopenings. At least in rich countries, we will probably get vaccinated a couple of times a year, against the latest variant in circulation, but never fast or comprehensively enough to achieve herd immunity.
https://www.bloomberg.com/opinion/artic ... t-pandemic
Opening schools and universities to face-to-face teaching, while teacher-age (or lecturer-age, or parent-age) people have been vaccinated but school-age and university-age children/youths haven't, for example.Chris Preston wrote: ↑Fri Mar 26, 2021 9:18 amI am not at all convinced this or will be the case. Most of the variants of concern arose prior to the vaccines being rolled. In almost all countries, there is still, insufficient people vaccination to put significant selection pressure on the virus.Herainestold wrote: ↑Thu Mar 25, 2021 12:45 amThe rapid rise of variants and rising infections in the face of vaccine rollout might mean we are now in a permanent pandemic where things will never go back to normal.
Most epidemics disappear once populations achieve herd immunity and the pathogen has too few vulnerable bodies available as hosts for its self-propagation. This herd protection comes about through the combination of natural immunity in people who’ve recovered from infection and vaccination of the remaining population.
In the case of SARS-CoV-2, however, recent developments suggest that we may never achieve herd immunity. Even the U.S., which leads most other countries in vaccinations and already had large outbreaks, won’t get there. That’s the upshot of an analysis by Christopher Murray at the University of Washington and Peter Piot at the London School of Hygiene and Tropical Medicine.Get used to masks and physical distancing and rotating lockdowns, closed borders, fewer pubs and restos, an absence of social events. The future is now.If this is the evolutionary trajectory of SARS-CoV-2, we’re in for seemingly endless cycles of outbreaks and remissions, social restrictions and relaxations, lockdowns and reopenings. At least in rich countries, we will probably get vaccinated a couple of times a year, against the latest variant in circulation, but never fast or comprehensively enough to achieve herd immunity.
https://www.bloomberg.com/opinion/artic ... t-pandemic
Variants are most likely to arise when the virus is being rapidly spread through the community, due to high virus populations. If vaccines are able to greatly reduce the population of virus being spread, then new variants will be much less likely.
Probably the biggest risk of selecting vaccine avoiding variants will be through vaccinating part of the population, but allowing the virus to spread freely among the rest. That will provide a scenario of high virus population regularly meeting vaccinated people...
I have the impression from over here that, apart from the usual gammon-faced arsed on the tory benches, there doesn't seem to be massive impatience to end the UK lockdown. What's the national mood actually like?Chris Preston wrote: ↑Fri Mar 26, 2021 9:18 amIt is a scenario we should try to avoid by not stretching out vaccination for too long and not opening up too soon.
Apart from London (11%), 15-19% of covid cases treated in hospital possibly caught it in hospital.One in seven patients treated for Covid between 1 August 2020 and 21 March got it while in hospital.
I've just plotted London's all cause deaths for 2015-2021, in my usual 4-plot format.badger wrote: ↑Mon Mar 22, 2021 2:21 pmIn the article he gives specific reasons for not using Den/Nor and non-Euro as comparators (mainly because of amount of international travel and/or climate), and am happy to go with that for the sake of argument and see what turns up...jimbob wrote: ↑Mon Mar 22, 2021 12:09 pmSweden, Denmark, Norway say that's bollocks.badger wrote: ↑Mon Mar 22, 2021 11:37 amApparently earlier does not necessarily mean better, when it comes to UK lockdown (because earlier first spring lockdown equals bigger second waves around winter, which, erm, could be prevented by, erm, earlier lockdowns?) Odd piece, seems to be no paper behind it:
Argues Cambridge Epidemiologist
And look at London in the first and second waves too
London - yep, that seems to run counter to his argument. Sweden, am not so sure - as I see it they had a slightly higher peak of excess death in second wave, so to me that also undoes his position, but he's really talking about countries which did well first, then didn't.