Woodchopper wrote: ↑Mon Aug 03, 2020 10:14 pm
bob sterman wrote: ↑Mon Aug 03, 2020 9:25 pm
shpalman wrote: ↑Mon Aug 03, 2020 9:17 pm
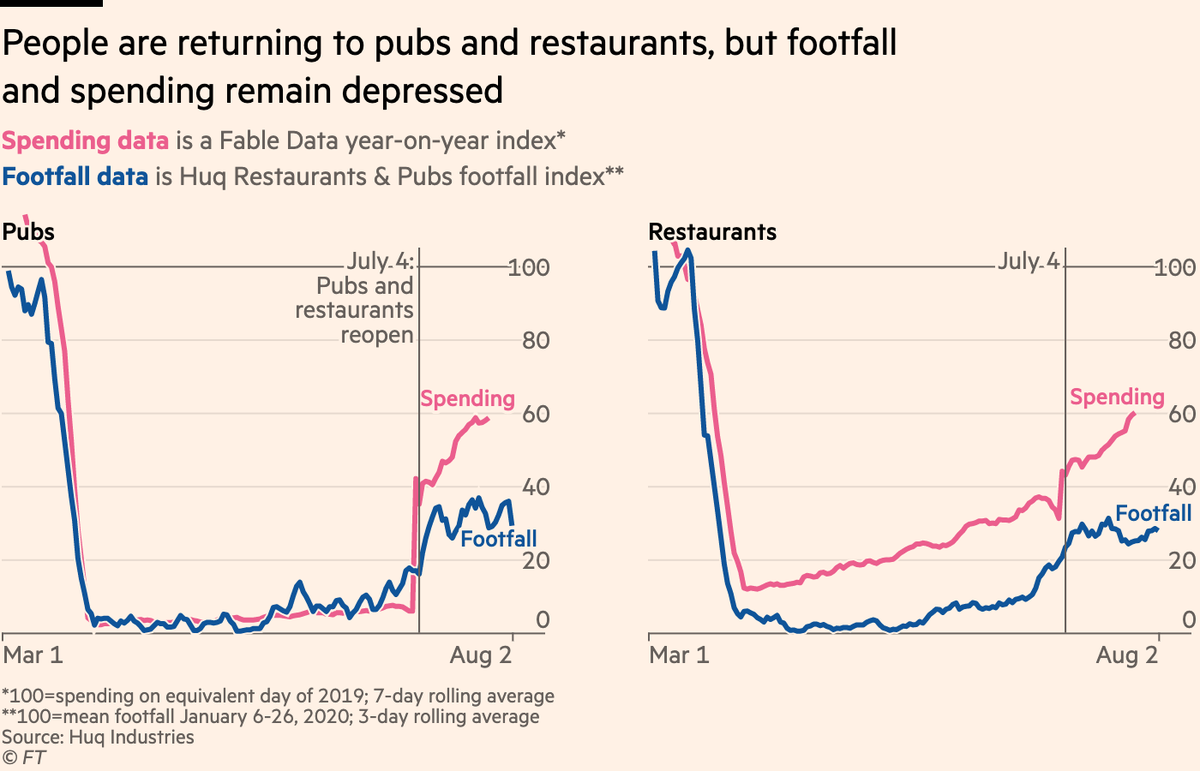
Results from mass antibody testing in Italy (a sample of nearly 65,000 subjects from all over Italy) would indicate that 2.5% of Italians had antibodies (that would be 1.4 million people, six times higher than the official number). In Lombardy, 7,5% which would be 750,000 people vs. about 96,000 official cases so far.
If there have been just 1,400,000 infections and if the reported total of 35,000 deaths is accurate - that puts the IFR around 2.5%. Close to estimates coming out of Wuhan early in the pandemic - but perhaps influenced by the the age structure of the populations affected in Italy.
Excess deaths were
48 600, which gives us an IFR of 3.47%, which seems too high.
Options seem to be:
a) many people who were infected don't have detectable antibodies any more.
b) something else killed thousands of Italians (maybe possible if the healthcare system collapsed and everyone else couldn't get treatment).
c) the sample is biased - for example if people who were sick are more likely to agree to be tested.
d) There was an IFR of 3.47%, which is what happens when the healthcare system collapses.
The excess deaths peaked here before the official covid deaths, in a way which suggests that in the early phase of the pandemic the testing wasn't keeping up with the actual spread of the disease. It's certainly possible that the health service was quickly overwhelmed in that period - there were 4000 covid patients in the ICU at the end of March, when there had only been 100,000 official positives of which 80,000 were still active (and two weeks later there were about 20,000 deaths). Right now there are something like 12,000 active positives, but only 40 cases in intensive care.
So it makes sense if there were actually about 500,000 cases of covid back when the official number was only 80,000.
The official protocol that a positive antibody test meant that you needed to go into self-isolation until you could get a negative swab test (at your own expense) was stupid. I don't think a person is shedding viable virus even if they do have a positive swab for viral RNA while also having antibodies and no symptoms.
The health service here also didn't really know what to do at the beginning. Protocol based on SARS was apparently to get people face-down intubated as soon as possible, and it was known that older patients wouldn't necessarily deal with that very well, so there was a sense of leaving someone at home as long as they weren't too bad, and when they suddenly got worse, oh well it's too late to do anything. We now know better how that works, with the decreasing blood oxygen saturation not necessarily causing any respiratory distress.
Italy also made the mistake of letting the covid get into care homes and hospitals (as well as the thing of extended families living together); 363 medical charts just have been seized by the police here in the province of Como because care homes are accused of manslaughter (and there is also an offense here of
epidemia colposa). (I'm not sure how that would map to UK law; "colposa" would mean someone was at fault but through negligence; "dolosa" would mean it was deliberate, but not premeditated.)
But how to we know what the IFR
should be?